
The Post Traumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5) is a 20-item self-report measure of the twenty DSM-5 symptoms of PTSD in adult populations (ages 18+). It is designed for use with people who have experienced traumatic events.
Consistent with the DSM-5, the four symptom clusters are represented in the PCL-5 by the following subscales:
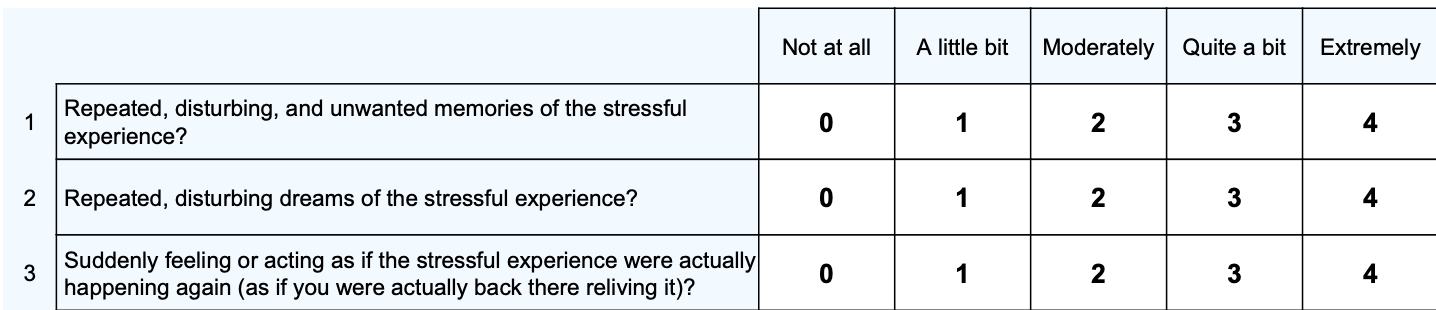
Example PCL-5 items:
The PCL-5 is widely used in clinical and research settings to screen for PTSD, assess symptom severity, and monitor treatment progress over time (Forkus et al., 2023).
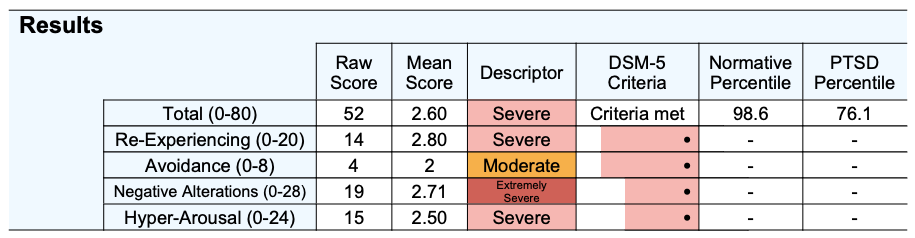
Scoring & InterpretationTotal scores can range from 0 to 80, with higher scores indicating greater PTSD symptom severity. Percentiles are also presented for the total score in comparison to both a normative and clinical (PTSD) sample. A normative percentile of 50 is indicative of an average score for someone who does not have PTSD, whereas a PTSD percentile of 50 is indicative of an average score for someone who is currently in care for PTSD.
There are four subscales which match the four symptom clusters for PTSD within DSM-5:
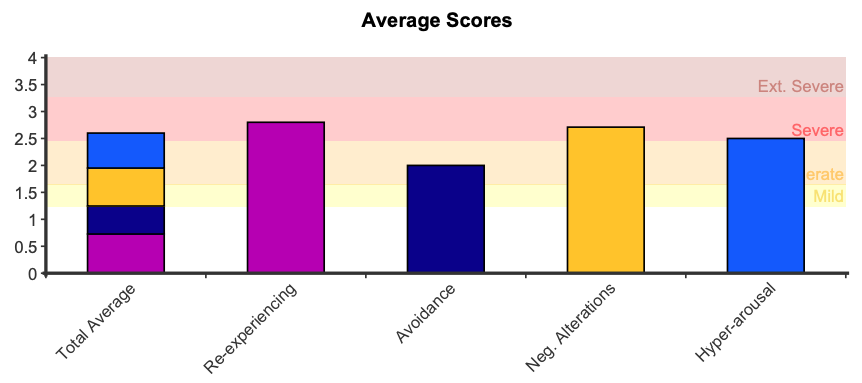
In addition to a raw score being presented, a mean score is also computed, which is the subscale score divided by the number of items within that subscale. The average score can help determine elevated symptom clusters when comparing each of the four subscales. These scores range between 0 to 4, where higher scores represent higher severity. Consistent with the likert scale:
Symptom descriptors are also presented for the total score and each of the subscale scores. These descriptors are determined by the distance from the normative mean:
Given the PCL-5 questions closely reassembled the diagnostic criteria in the DSM-5-TR, a provisional PTSD diagnosis can be made based on the following rule. The DSM-5 diagnostic criteria requires at least: 1 Criterion B item (questions 1-5), 1 Criterion C item (questions 6-7), 2 Criterion D items (questions 8-14), and 2 Criterion E items (questions 15-20). A score of 2 (Moderately on the likert scale ) or higher is an endorsed symptom.
Notwithstanding the DSM related diagnostic criteria, scores of 33 or above are considered to be of clinical significance, and can serve as an alternative threshold for identifying significant PTSD symptoms that interfere with daily functioning (Bovin et al., 2016; Krüger-Gottschalk et al., 2017; Rosendahl et al., 2019).
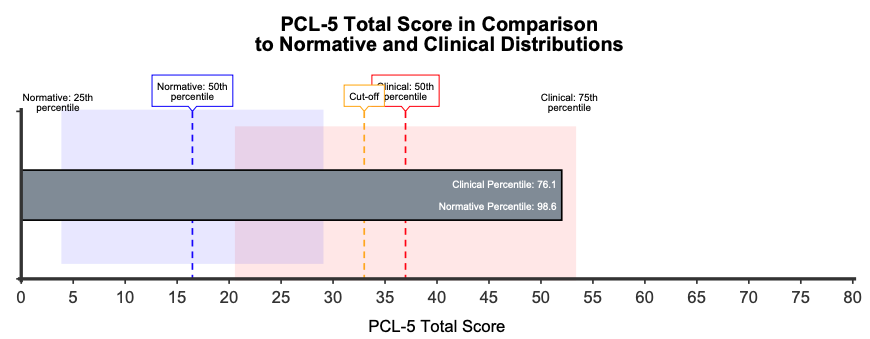
A comparison graph is presented showing where the respondent’s score sits in comparison to the normative and PTSD samples, with shaded areas around the means indicating the two middle quartiles (between 25th and 75th percentile). This graph can help contextualise PCL-5 total scores in comparison to the distribution of responses among clinical and non-clinical groups. A cutoff score of 33 indicates the point at which symptoms are defined as clinically significant.
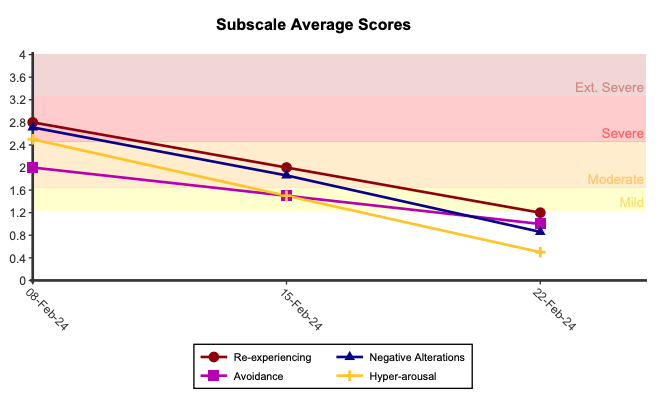
When administered more than once, longitudinal graphs are presented showing change in symptoms over time. A 12 point change during the course of treatment represents clinically significant change (Renyer, 2016).
Psychometric PropertiesA review of the PCL-5 using 51 studies demonstrated that the internal consistency for the total score ranged between .83 – .97 (Forkus et al., 2023). Test-retest reliability was tested across a range of time intervals and was found to range between .58 – .91 (Forkus et al., 2023). The PCL–5 total score showed moderate to strong correlations with other measures of PTSD (.44–.89; Forkus et al., 2023). Construct validity was assessed using group difference tests. Individuals with PTSD (vs. without PTSD) had a significantly higher PCL–5 total score (Fung et al., 2019) and individuals with probable PTSD (determined using recommended cutoff scores) had significantly greater mental functional impairment compared with those without probable PTSD (Forkus et al., 2023).
The normative percentiles are calculated from a combination of a non-clinical, non-trauma exposed group and a non-clinical but some trauma exposed group (N = 166, M = 16.47, SD = 16.29; Renyer, 2016). This group was combined to provide a more realistic non-clinical group where some of the group may have experienced some trauma (but not have PTSD) and some of the group have not experienced any trauma at all. Renyer (2016) also determined a reliable change score of 12. The clinical (PTSD) percentiles are calculated from a sample of military veterans in clinical care for PTSD (N = 468, M = 36.97, SD = 21.16; Bovin et al., 2016).
The distance from the normative mean described above was used to produce symptom descriptors: